In 2024, Caret Health deployed its clinical tasking platform at a large health plan in Nevada. The health plan wanted to improve control of diabetes and hypertension in its high risk patient population.
Caret Health’s platform cohorted patients based on the following actions:
Identify each patient’s technology literacy
Create path-of-least resistance clinical pathways for each patient
Optimize outreach based on each patient’s individual communication preferences
Subsequently, the Nevada health plan launched a Caret Health utilization management program that included:
Patient outreach, education, and consent
Chronic care management
Remote patient monitoring (biometric monitoring devices)
Patient alert, triage, and escalation pathways
The clinical staff utilized Caret’s executive management and clinical tasking systems - powered by the caretEngine.



Triage and escalation pathways
The study cohort comprised 954 patients who were enrolled in the utilization management program. Caret actively monitored their vital signs daily via remote patient monitoring and engaged in chronic care management for 6+ months. They were also subject to alert, triage, and escalation workflows as appropriate.
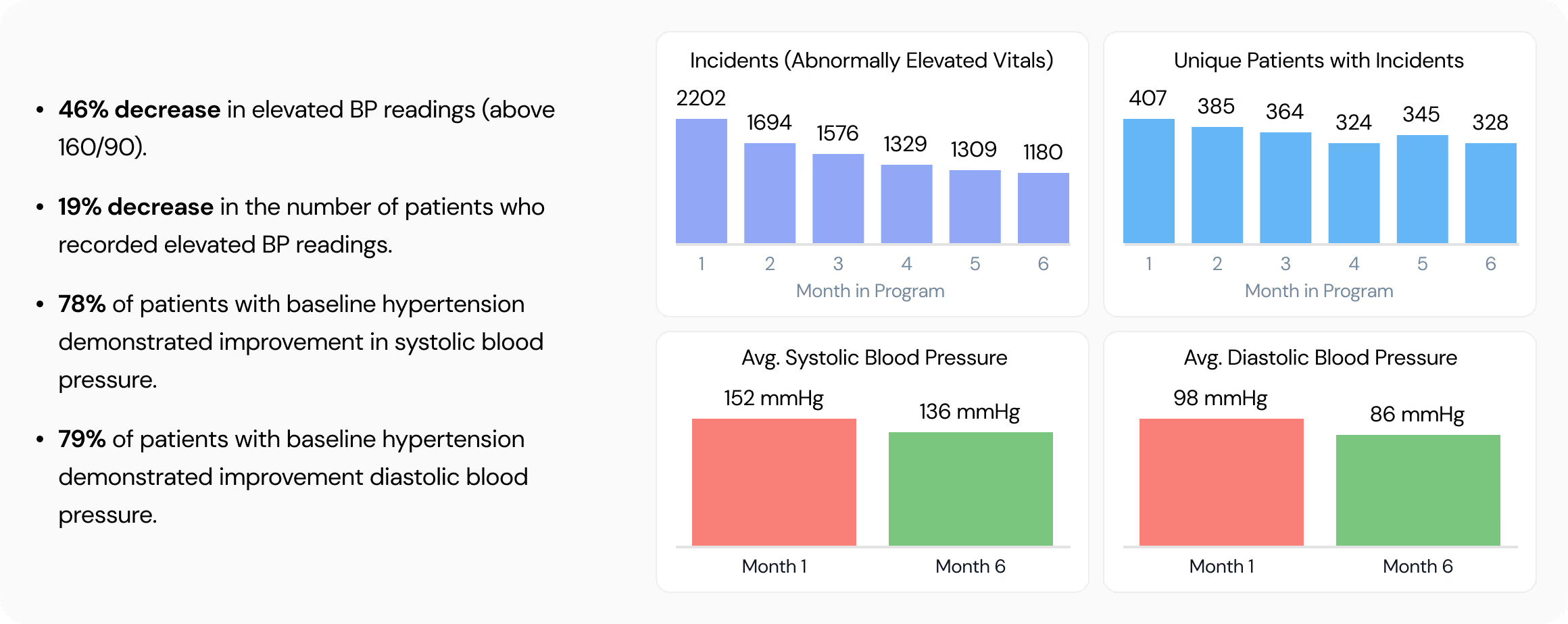
Results
Over the course of 6 months, Caret Health’s interventions led to a significant improvement in blood pressure and glucose control. Specifically, there has been a more than twofold decrease in the frequency of abnormally elevated vital sign submissions on a monthly basis. Patient engagement and adherence persisted over the intervention period.
Among the entire population cohort of 954 patients in a 6-month period.






Among the entire population cohort of 954 patients in a 6-month period.


Claims data processed for these patients show that the utilization management program has generated >35% reduction in all-cause hospitalizations and ER visits.
Detailed clinical information and process summaries are available upon request – please contact info@carethealth.com or visit www.carethealth.com to learn more


